There is a service for virtually anything you want to do digitally. As a practical example, every EMR or EHR has data entry quality challenges that have significant impacts on costs and human interaction. One such example is the use of email in a modern medical office. We use email for reminders, patient communication, collections, just to name a few, and entering the wrong data, in the beginning, can cause a lot of extra work and headaches.
It’s a big deal to have email entered correctly at the first attempt because email is a vital pipeline to communicate from that point onward. Fortunately, it is a problem that is easily solved using existing online services. There are hundreds of email validation services available online and most have well-documented APIs. We chose an API that is widely used and allows 100 validations per day at no charge. Yes, there is absolutely no charge for doing small amounts of email validations per day yet it will save your staff hundreds of hours of time over a year.
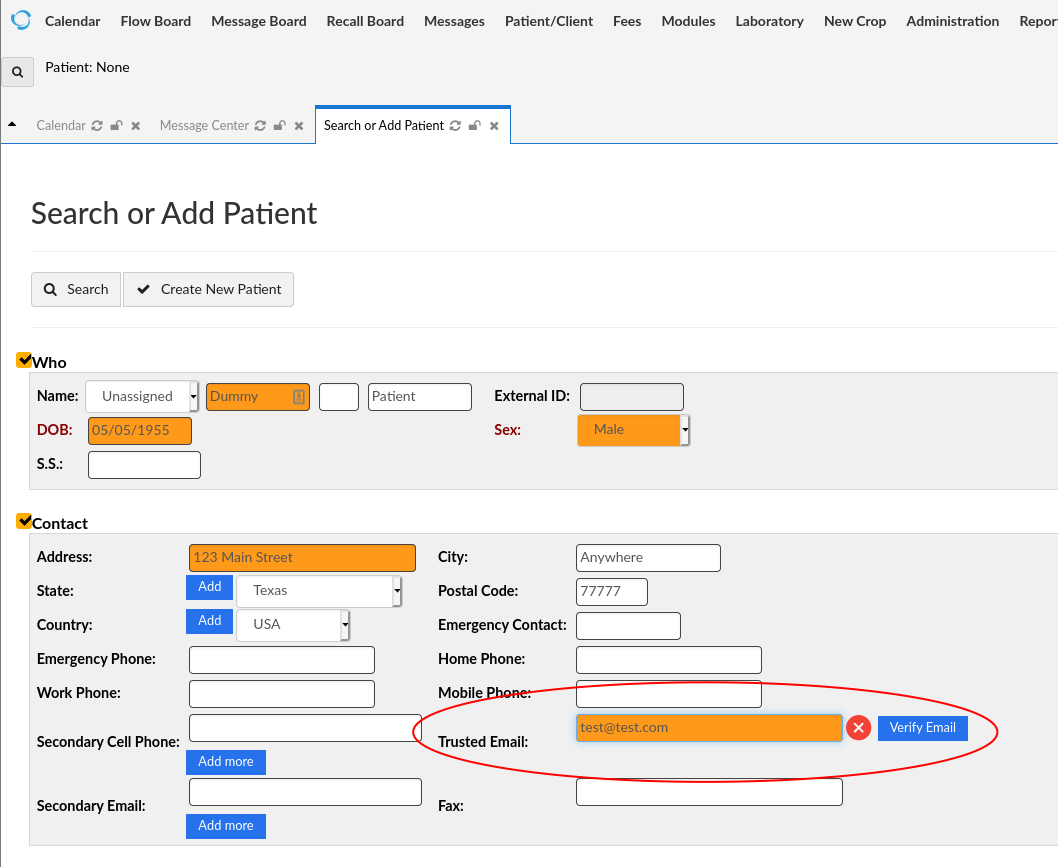
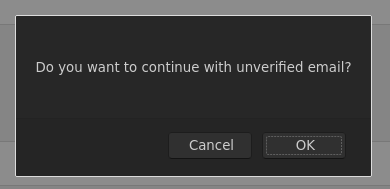
In general, you need to validate/fix data at the point it is entered into your systems. Our OpenEMR email validation integration uses this principle by requiring the EMR user to validate the email for a new patient before saving the new patient information, otherwise, a “warning” popup indicates that the email has not been verified and that should be done before saving the new patient data.
The email validation service is not perfect as not all email providers reply with an accurate email validation but we have found it to be better than 90+% accurate which has yielded a 75% reduction in incorrect email addresses being entered into your EMR. This integration was not available as part of the core OpenEMR system but was only a couple of hours of effort for a qualified programmer with OpenEMR experience. This is a great example of a cheap, easy, HIGH-impact customization to OpenEMR.
We are firm believers in open-source, community-supported software. For most industry-specific software, once the basic use-cases are addressed and the basic feature set is completed, most development time is spent on use-cases that do not address the broad-based needs of the user base. In other words, it is similar to the 80/20 rule where 20 percent of the feature set in a mature software product will address 80 percent of the needs of the users. Why pay for a high-priced software license when most of the software vendor’s overhead is spent developing features that do not address your needs? Open-source software, like OpenEMR, gets you 80% of what you need, without the high-priced license, with the ability to customize for exactly what your office needs regarding features and workflow. Imagine having software that is formed for you instead of having to change your procedures and policies to fit the software product you have adopted. Maybe it’s time for a change?
Full Transcript:
Jon Pafk:
Hey guys, my name is Jon Pafk, and this is Brent Boecking. We are two of the dudes behind Vital Healthcare, and we’re starting our first edition of, what we’re going to call, Health Tech con Carne. Since we’re both barbecue fans, we’re going to be dishing out some meaty details on how healthcare tech can, in our own opinion, evolve to make practices a lot more intelligent and make patient experiences a whole lot more enjoyable, maybe as enjoyable as stepping into your favorite barbecue joint, hence the picture behind me of the old Franklin barbecue tray. So, we’re going to cover the latest in healthcare tech, plus maybe review or talk about one of our favorite barbecue joints in this.
Jon Pafk:
We’ll keep this short, but in this one, we’re going to be talking about patient communication and specifically an oldie, but a goodie… fax machines… not that oldie and definitely not that good. So, actually let’s talk about email, Brent. So, one of the most common platforms in all patient communication is email. I’m not sure if we even have a number in terms of the number of emails that we send in a day, week, year in our practices, but what happens when you’ve got the wrong email? And so, we see it all the time, the patient wrote it down wrong, staff entered an email address wrong, maybe a Gmail without the G, we see that, or the Yahoo with an extra O. So, it’s a common mistake. So Brent, how is email used today in our practices?
Brent Boecking:
Well, it depends on what your consent system is like. You can do a lot of things if you get consent from the patient to do it. And the practices that we’re involved with, obviously we work on making sure that they’ve got a pretty robust consent to be able to share information with the patient via email, or else you’re somewhat limited. But at any rate, if you have a pretty robust consent, you can share a lot of stuff via email.
Brent Boecking:
Beyond high-tech techniques like Slack and otherwise, the everyday man is using email as their primary mode of communication. Heck, I mean, the majority of us communicate with our grandparents or our parents via email now, and it’s no different for patients. We use email communication to initially remind them about their appointments, tell them where the paperwork is that they’re going to have to fill out, or at least initiate them on the journey to start filling out the intake information that we need.
Brent Boecking:
There’s a lot of tech around that as there should be because it’s one of the least efficient things that we do. So, we use it for reminders, we use it for general communication as well, just back and forth. There’re other methods as well for that, but email is fantastic. For instance, if people want their records and they’ll consent to get the records via email, we can send records. And you brought up faxes, faxes are still dominant in the medical space, unfortunately.
Brent Boecking:
I remember the days when I had a fax in my house. Thank God those days are over, but you will find a fax machine in every single medical office in the United States anyway. Probably not in other countries, because they’re smart enough to use email, but in the United States you still find faxes in every lab, every medical office, every hospital, cause it’s one of the dominant, if not the dominant way to transfer information from practice to practice. What are some other ways that we use email? We use email on a lot of ways like newsletters. [crosstalk 00:04:24] I don’t know how thorough you want to be, but it’s our primary and dominant mode of communication, is to use email.
Jon Pafk:
Yeah. So, we have appointment confirmations that often trigger through email. And we’ll talk about it in another episode, about texting and the power of texting. A lot of back and forth with patients, referral sources, etc. with email.
Brent Boecking:
Yeah. And it’s rapid too, right? And it can be handled. And we all know this about email, but maybe we don’t think of it in terms of communication within a medical office. But phones are tough because they have to be on-demand. So, if you call there has to be made a connection in real-time. Whereas email, at least there can be minutes, 15 minutes, 20 minutes, 30 minutes, and there’s an expectation that if somebody gets back to me in an hour or even six hours, that’s a reasonable amount of time. So, email doesn’t necessarily always interrupt you from what you’re doing, but yet it’s still a relatively rapid form of communication, which is really nice. And so, patients feel like they’re being taken care of in a relatively fast manner.
Jon Pafk:
Yeah, absolutely. It’s still the large majority. I don’t know. I don’t really have the data, but probably the largest majority of communication. Although, if I had my way, I’d love to retire from email, but it’s just the way that life has gone now.
Brent Boecking:
As a practice for us, we probably … And when I refer to the practice for us, I’m referring to Pro-Care Medical Center. Pro-Care Medical Center probably sends in the order of a couple 100 emails, just appointment reminders a day, much less than any of the other email that comes in and out. It’s hundreds a day, it’s thousands a week just for the small practice of Pro-Care medical center.
Jon Pafk:
Yeah, absolutely. So, it’s pretty crucial that we have the right email addresses, but occasionally errors do occur. So, what are the common mistakes that we see with email entry at Pro-Care through some of our clients?
Brent Boecking:
So, data entry is a big thing. It’s hard enough to understand people on the phone, because again on a phone call, you have to make that point-to-point connection in a very short amount of time. And in medical practice these days, the majority of new patients still come via phone calls. And so, there’s definitely an impetus to get to every single phone call within a very short amount of time, because you don’t want to lose out on new patient volume. And so, you have to slow down around the time that you’re getting the email, because you can get their address wrong, you can even get potentially their date of birth wrong, you can miss spell their name. But if you misspell their email address, you’re missing that crucial link for those first primary communications with the patient, which is a big deal.
Jon Pafk:
Yeah. And you mentioned sometimes it’s hard to understand someone on the phone a lot of times. And I know I’m occasionally guilty of this, although you and I both have unique names, spelling or saying our email address maybe a little too fast. And so, you and I were talking a little bit about best practices. What are some of the things that we’ve done operationally to ensure that we’re getting emails right?
Brent Boecking:
You’ve got the practical things, which practically speaking, we impress upon the people that answer phones, which really a lot of times can be just a few people in a practice, or it can be just about anybody in the practice, depending on what practice you’re running. But, if it’s anybody that’s going to answer the phones, you have to impress upon them that they’re going to have to slow down when they get to the email address. Again, it’s fast and then it’s slow, and you’ve got to be slow and you’ve got to be deliberate.
Brent Boecking:
Honestly, it’s very nice to be able to have the aviators’ alphabet at your disposal if it’s something that you do a lot, because then you can repeat it back to the patient, or you can have the patient repeat it back to you. I find its best when the patient tells you, and then you repeat it back to the patient letter by letter. It’s really important that it’s letter by letter, because otherwise it’s like Brian, is it B R I A N or B R Y A N? And you just gloss over it and just assume it’s right, and then you end up getting a wrong email in the system, and you’ve at least broken the chain up until the point that they come in and you get their paperwork.
Jon Pafk:
Yeah. Especially with a lot of common names, that can be a challenge too, where you’re maybe communicating, you’re confirming appointment details that are going out to a completely different person.
Brent Boecking:
Yeah. And that’s an incredibly awkward situation, and you’ve got to be pretty expedient about fixing it.
Jon Pafk:
Absolutely. So, there’s definitely some risk involved from getting that wrong. So, we’ve talked a little bit about channels like bones. We see online appointments being booked, and that’s even the patient putting their email incorrectly, occasionally with chat. Any other channels that you commonly see? Obviously, phones are probably the biggest one, but ultimately how does it impact patient experience with correct or incorrect email information?
Brent Boecking:
The incorrect email is a big deal, because again, your no-show rate on somebody that doesn’t get a confirmation via email, it’s got to be double or triple, compared to somebody that’s gotten an email validation or verification, that it’s “Yes, you do have an appointment at this time with this doctor at this location.” How many times in practice do you see, especially multi-location ones, that somebody shows up at the wrong location, because their anti-phishing or antiviral software blocked the email? It’s a big deal. It’s a big deal to get it right.
Jon Pafk:
Yeah. And we’ll talk about this in probably another episode, of the importance of multi-channel communications to your patients. But certainly, as we’ve established, emails are probably still your most common and most expected way to receive confirmations. Patient relationship management, obviously that’s a big thing for any clinic. And in the business world, we talk about CRMs or customer relationship management, patient relationship management inside clinics. How does email play a role in that?
Brent Boecking:
Well, again, it’s the primary mode of communication. So, when you’re wanting to communicate to patients that you’re going to be closed for a holiday, or that you’re running, or you want to say hi. Say that you want to de segment your veteran population and send them a specific “Hi, happy Veterans’ Day.” And potentially some offer with regard to that, that’s really important. And again, if you don’t get an email right, you’re not going to get the opportunity. There’re a lot of mechanisms for being able to correct an email, but none of them are that great. It’s way better to get it right in the first place.
Jon Pafk:
Yeah. Especially with, you mentioned the first impression. Especially if you’re getting emails, maybe first not getting an email. Second, it’s got the wrong information included in it. But patient relationship management, when we talk about that first impression, especially with being able to welcome a patient, hit them with additional information on how to get in touch with our clinics directly, other services that we provide, and just try to be as much of a helpful resource through email communication, so that emails from Pro-Care are valued versus seeing another email from Pro-Care and it’s just another form of spam.
Brent Boecking:
Yeah. As you know, that’s really important that your communications are valuable, because otherwise why are you bothering to send them? But as long as you’ve sent high-value communications, obviously like patient reminders, they’re pretty high value. And then along the lines of maintaining that relationship with that patient with good information. You don’t want to send, “Hello, it’s Monday and the weather’s this.” And their email on Monday, Tuesday, Wednesday, Thursday, Friday, because eventually just won’t look at your email.
Jon Pafk:
Yeah. And so, we’ve established obviously the importance of email communication inside healthcare practices. And it’s obviously an issue in terms of getting the right information plugged in for the right email addresses. So, what’s a practice to do if it’s an issue? And we have enough history where we’ll honestly say, “Yeah, it was an issue for us.” How do you manage that today? What are some of the best practices?
Brent Boecking:
So, what we started doing is, you always start … In any system where you’re entering data, you always want to start with the inlet. The inlet is the most important piece of any system that’s driven by data, whether that’s your electronic medical records and your doctor entering that data, or if it’s talking to patients and it’s email addresses. And so, we address the beginning. And for instance, at Pro-Care, we’ve got a pretty small subset of folks that answer the phones. And so, we counseled them on exactly what verbiage we wanted, as far as them getting emails. First of all, them understanding the importance of getting the emails is what solidifies it in their mind, because if they understand why then they typically will continue to follow the steps.
Brent Boecking:
If they don’t understand why you can tell them that it’s important, they get emails all day long, and whether they actually do it or not is another thing. But if they understand why, and they get appointment verifications, they get our newsletters, they potentially get doctor results, documentation, this, that, and the other. Then when they know that, and they understand how important it is, they understand that they do need to slow down and make sure that they get the patient information in there. And so, we talk to the folks that are primarily answering phones. And then, also when you get something wrong, it’s also important that you fix it. And so, we monitor all of the bounce back on email, and we actually have a process scoped for fixing them.
Brent Boecking:
And so, one of the first things that we do, is we go check. Say that they’ve already been in to see us, and we’ve got a bounce back, we’ll go in and check the new patient paperwork versus what’s in the system. And if that looks like it matches, or if their handwriting was so poor that we couldn’t read it, or we couldn’t verify it, then we’ll go to actually sending them a text. So, assuming that we’ve got the ability to text back and forth, and usually by that time we do, most people do communicate via text. We’ll text them and say, “Hey, this is the email that we’ve got on file. Is this right? Or is it wrong? Can you update us on the email?” And so, if that doesn’t work, we generally don’t go to the step of actually calling them or sending them a letter or anything like that.
Brent Boecking:
We will mark it as that email’s not a viable route of communications. But something else that we’ve done specifically, which is what a lot of the blog entry talks about, is the actual guts of email validation. There’re a bunch of services online that do email validation. And so, there’s this thing called an API, which is just nerdy talk about machines talking to machines in an efficient way. And so, they’ve got these email validation APIs, and there’re bunches of them out there. The one that we ended up using allows us to validate up to 100 emails a day, which is fine for most practices. Obviously, if you’re running a high volume hospital, that’s not going to be sufficient.
Brent Boecking:
But it works. It’s going to work for 90 plus percent of practices out there, to be able to do up to 100 email validations a day. And so, as you’re entering a patient’s information into our electronic medical records, we’ve actually added a button that grabs the right email address and goes to validate it against an external system, and then furthermore pops up. If you don’t do it, it pops up a warning. When you go to save the patient’s information it pops up a warning and says, “Hey, you didn’t run an email validation, are you sure you want to save this data?”
Brent Boecking:
And so, you can still bypass it, which is also important that you can bypass quality control systems, but you want to make it to where there’s at least a red bump to bypass the quality control systems. Because, say that they did give you a bad email address or that English was not their first language, and you’ve tried to ask them seven different ways to what their email address is. You’ve spelled it, you’ve listened to them, you’ve tried different ways and you’re still not getting it, you need to be able to bypass it.
Jon Pafk:
Yeah. And there are even patients that will provide you a dummy email address.
Brent Boecking:
That is correct. And also email validators are not perfect. Hotmail is a specific one that basically will validate everybody. You can just stick any crazy email you want @hotmail.com and it’ll validate all of them. So, not all email validations work perfectly, but I will tell you, in our systems, when we initiated this email validation, our bounce back went bound by probably 75 to 85%. And when we get to where we send out statements, there’re just a handful of bounce backs into the thousands of statements that we send.
Jon Pafk:
Yeah. So, coming back to practice growth and patient relationship management, all of a sudden you’ve got so much more efficient in terms of, one, the way that you’re communicating, and then two, the rigor that it used to take to follow up with patients on the statement or a bill that was emailed, and they removed a whole lot of stuff.
Brent Boecking:
It’s multi path. Our deal, even though we’re talking about email, is you want to communicate with your patients the way they’re comfortable communicating, whether that’s email or whether that’s text or whether that’s phone. And then, companies like Twilio are coming out with some really neat stuff where it’s really the same interface to be able to interface with WhatsApp and potentially Facebook Messenger and a lot of other ways to communicate with people too, to where again, the idea is that you want to be able to communicate to them, and the way they want to communicate to you.
Brent Boecking:
And that also includes web bots or not web bots, but a webchat. Maybe they’re most comfortable going onto the web and chatting with you that way. You don’t want to force them into the way you want to communicate as a clinic, you want to communicate to them in the way that they want to communicate to you. But also, on the flip side of that, you have to make it simple for your staff, because you can’t have your staff checking 17 different portals of 17 different ways to communicate with patients. That’s just terribly inefficient.
Jon Pafk:
We’ll probably talk about patient communication and HIPAA in another episode. But, email and having really, for any data, making sure that it’s accurate drives a tremendous amount of goodness in terms of practice operations. And so, that’s keeping it super clean. You hit upon this.
Brent Boecking:
Another point, Jon, is freeing up your phones for the things that we talked about. Still, the majority of new patients come in via the phones. And if you can divert a bunch of that non-new patient traffic off to email or text or some other mechanism, you’ve got fewer people that have to man the phone. So, it’s a cost-saving manner or mechanism. And then two, you’ve got a better chance of actually picking up the phone call, because the first person that’s going to hang up in the shortest amount of time possible, is a new patient. An existing patient is going to sit on hold for a little while, you’ve already captured on. It’s the new patient that is going to be completely, maybe not completely intolerant, but they’re going to be somewhat intolerant to waiting.
Jon Pafk:
Yeah. Well, again, we talked about the importance of first impressions, and you spend a whole lot of time waiting on a real person to answer the phone call. It may give you an idea of your experience once you get into the practice. So, the tolerance is super low. You hit upon this, but really, how does Vital solve for email validation? You’ve talked a little bit about the tools and the systems.
Brent Boecking:
So, one of the things with Hey Vital or Vital Healthcare, is that we have adopted what’s called open-source software. So, it’s licensed software, but we don’t charge for the license for the software. The source code is freely available online. The secret sauce is to make it all make it work, and make it all play together. And so, we use an open-source EMR called OpenEMR, which we have found to be fantastic. It solves that purpose of industry. Industry-wide software, you spend, especially industry-specific software, if you’ve got a vendor that’s supplying you software, say it’s an EMR, 80% of their …
Brent Boecking:
Well, let’s say this, they spend 20% of the time giving you 80% of what you need. So, they came out with this product, it’s got all these basic features and those features address their entire population of the people that use it. They spend, after that initial feature set, they spend the entirety of their development time usually working on things that less than 20% of their audience is even going to need. And so, you pay for these developers to develop things that you’ll never use because it doesn’t fit your workflow, it doesn’t fit your clinic needs, for whatever reason, it’s not for you. The great thing about open-source software in general, and specifically OpenEMR, is it’s got a really great basic set of features.
Brent Boecking:
It’s got a calendar that works very well, it’s got a basic set of templates, it’s got a really easy-to-use workflow, it’s got connectivity into billing and collections and all that stuff. Specifically for us, being Vital Healthcare, is that we’ve made the EMR talk with a bunch of other stuff, which makes it even much more powerful than just an EMR. Marketing automation, telephone systems, etc. The amount of connectivity is pretty impressive. But specifically with regard to email validation, we just added … It was less than stars, lights, all those stuff.
Brent Boecking:
It was less than half a day of development time. It was probably three hours of development time, to find the API, the email validation API that we wanted to use, add the button to the new patient addition screen in OpenEMR, and make a little pop-up warning happen if you don’t do it, or if you try to save it without validating the email. That was literally probably three days, sorry, not three days, probably about three, maybe four hours of development time. It was an absolute no-brainer, and it’s had huge returns.
Jon Pafk:
Yeah, absolutely. The OpenEMR ecosystem and using the open-source API is to be able to just build a frank and robust system, but some of those small little improvements, those incremental improvements that were fairly small level of development investment, that just had a huge payoff in terms of return. And that’s really one of the reasons that we wanted to start with email validation, because it’s one of those little things in there, but it can be a huge hassle when you’re not able to be able to communicate effectively to your patient base, your patient growth, your patient relationship management, but being able to solve for that, and solve for that fairly quickly and easily.
Brent Boecking:
Yeah. And the alternative is, if it’s something that you’ve dreamed and you’re like, “You know what, it would be really nice to have email validation.” But say that you’re tied in with one of the non open source vendors, there’re hundreds out there for EMR, and you were like, “Hey, I would like to have this feature added.” Number one, you probably don’t even know who you would ask to have the feature added, because you’re probably not asking for a bunch of features. They’re not even asking you to add a bunch of features depending on how mature the product is.
Brent Boecking:
And even if you were able to talk to somebody, you’ve got to get on a roadmap to be able to get your feature added. And in the experience that I’ve had with multiple, probably half a dozen EMR vendors, the likelihood, even one that’s not necessarily very mature, the likelihood of even getting something simple, where it takes three development hours to get it implemented, it’s probably not very good that you’re going to get it at all. And it’s certainly not very good that you’re going to get it in a short amount of time.
Jon Pafk:
Yeah. I like to joke, but we’ve taken the Tesla approach to development at Vital, right? You get some feedback, whether that’s through employees or with your patients, or whoever’s using the tools and technology to run the plant, right? Get that feedback and maybe deploy a fix pretty quickly or deploy a feature pretty quickly. New bells and whistles that a lot of the Tesla’s see after some feedback that Elon gets via Twitter and stuff.
Brent Boecking:
That’s serious. That is the world that we live in to get today outside of healthcare. Even our cars get over-the-air software upgrades if you’ve got a Tesla. I think everybody else is scrambling in the car industry to catch up. And I think you’re right on. I think people should expect some level of rapid improvement based on … 80% of what clinic to clinic does, is the same, but there’s that other 20% that when you adopt an EMR, that doesn’t work for with how we do that. How do we do that process right now? And so, the general consensus is, that when you adopt an EMR, you’re going to adopt their workflows.
Brent Boecking:
Certainly, their workflows are not going to adapt to you. And I think that’s a bit different when you’re looking at something that’s open-source, because you can certainly make the workflow adapt to you, and what works best for your clinic and your demographic of patient, and the type of patient you have. Whether they’re cash, they’re major medical, they’re on some subscription plan, you do comp, you do personal injury. There’s a lot of different ways to deliver medicine, and some of them are employers, that’s yet another one. And the workflow of each one of those is 80% the same and 20% different, but that 20% difference will break a lot of systems. They just literally cannot accommodate it. It can’t accommodate it on the intake side and it can accommodate it on the billing and collection side.
Jon Pafk:
Yeah, absolutely. We’ll go into a whole lot of those as we build upon Health Tech con Carne. But I think to wrap up, we were talking a little bit about this before we jumped on and started recording. What’s the email validation equivalent for barbecue for you?
Brent Boecking:
What did we say? It’s the beans? The quality of the beans?
Jon Pafk:
Right, yeah. A lot of barbecue joints in Texas have free beans, right?
Brent Boecking:
That’s right. It better be good.
Jon Pafk:
Yeah, it better be good.
Brent Boecking:
It’s the Canary in the coal mine for the barbecue joints. Is this place going to kill me or not?
Jon Pafk:
Yeah. So, we’re two Texas boys, born and raised. Obviously big barbecue fans as well, and spent a lot of time in health and health tech. But to wrap up, your favorite barbecue joint, we’ll talk, or maybe pick a handful to feature and highlight, but is there one that you’d want to shout out in this first episode?
Brent Boecking:
I like Stiles Switch down the road. Their sausage is the absolute best I’ve ever had probably anywhere.
Jon Pafk:
Yeah. It’s pretty good. My background at least has a little bit of a note to Franklin BBQ. And there’s a reason that he was the King of Texas barbecue. A lot of folks have certainly followed his wisdom. Great dude. Amazing barbecue. It’s been awhile though since I’ve had a chance to enjoy it.
Brent Boecking:
We’ll have to send this to Franklin and see if he enjoys our email validation talk.
Jon Pafk:
That’s right. That’s the least of his concerns. Just trying to make some good beans. Well, good stuff. We’ll go onto the next step. Hopefully, we’ll keep this rolling and keep featuring some specific features or technology issues that all clinics run into. And some of the health tech fixes on the way that can help make their lives a little bit more interesting and certainly clinics run a whole lot more efficiently, so good stuff.
Brent Boecking:
Awesome. Thanks, Jon.
Jon Pafk:
Yeah. Thank you.